B18. 2026
B16. 2023
B13. 2018
B14. 2019

B12. 2016
B11. 2014
B9. 2010
|
Overview: Rolls
has made discoveries about the brain bases of mental disorders that
have their foundations in his interests in emotion and in computational
neuroscience (B16, B18). Rolls and colleagues
have discovered that depression can be related in part to increased
connectivity and sensitivity of the non-reward related lateral
orbitofrontal cortex and decreased connectivity; and reduced connectivity and sensitivity of the
reward-related medial orbitofrontal cortex (626,
B13, B16, 679, B18). Rolls and colleagues have
related the symptoms of schizophrenia to altered stability of cortical
attractor networks (631, 629, B18),
in turn related in part to reduced forward relative to backward
connectivity in the cerebral cortex (602).
These approaches have been extended to the memory changes in normal
aging (540),
to autism (541, 609),
to obsessive-compulsive disorder (449), to ADHD (629), and to the emotional
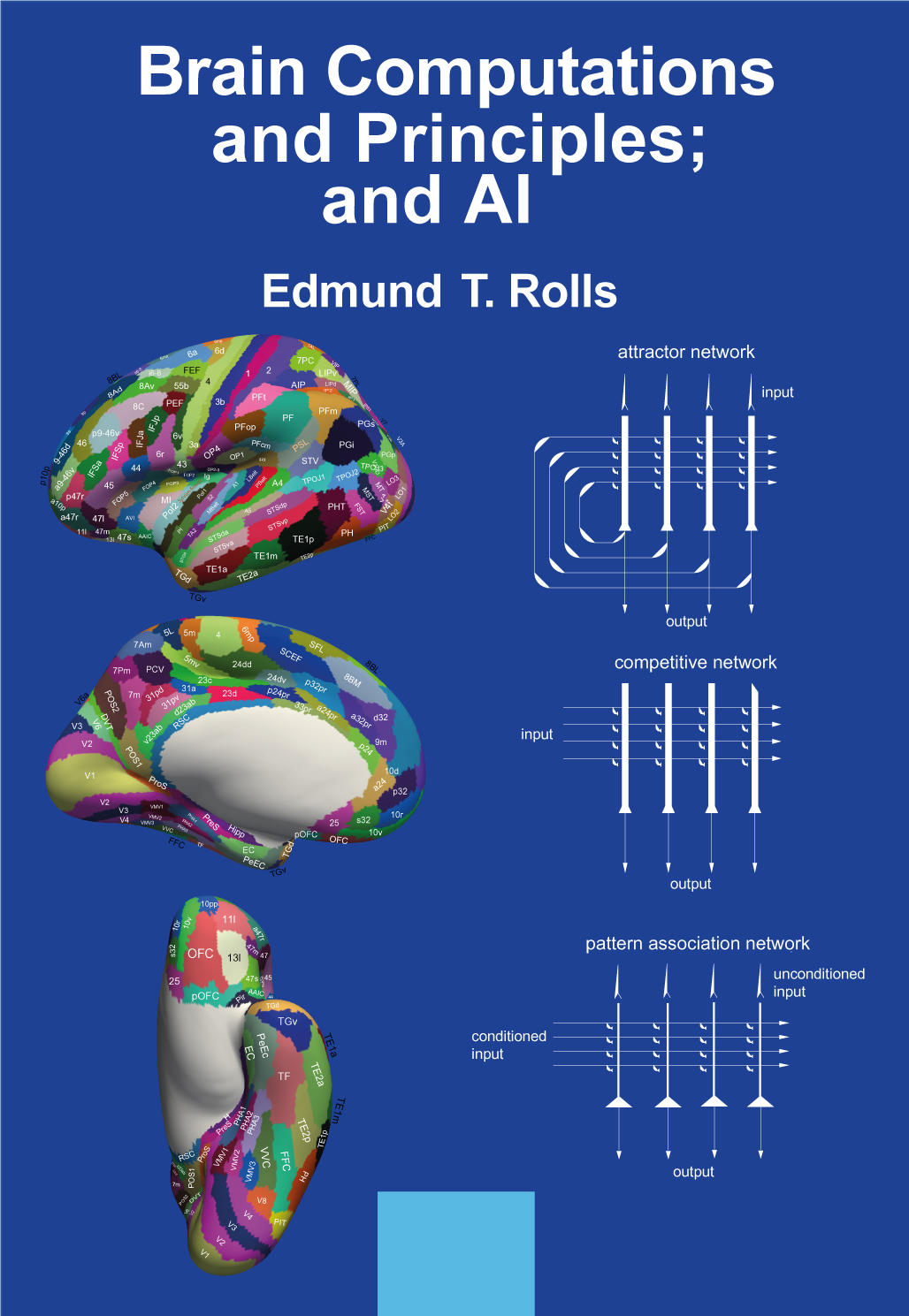
changes that follow brain damage in humans (641, B18). A key publication describing these discoveries is Brain Computations and Principles; and AI (B18).
Depression
A
non-reward attractor theory of depression, in which the lateral
orbitofrontal cortex attractor network system for non-reward maintains
its activity for too long; and the medial orbitofrontal cortex reward
system is less responsive (559,
572, 579,
626, 679, B12, B13, B14, B16, B18). The theory
is supported by a model of the computation of non-reward in
the orbitofrontal cortex (562).
An introduction to the theory is available as a lecture.
The lateral
orbitofrontal cortex and adjoining inferior frontal gyrus (615)
in depression has increased functional connectivity (564, 591, B14, 626, B16, B18) with
the precuneus (where the self is represented, and which may contribute
to the low self-esteem in depression) (592);
with the angular gyrus (involved
in language, and which may contribute by a long loop attractor to the
negative rumination in depression); and with the temporal lobe cortex
(which may contribute to the sad interpretation of faces and
events) (564).
Effective or directed connectivity from the medial orbitofrontal cortex
to the lateral orbitofrontal cortex is increased in depression, and
given that the activity in these areas is reciprocally related, this
may release the lateral orbitofrontal cortex into high activity, which
was found in the analysis (583).
Rolls' theory of
depression (559,
626,
B13, B14, B16, B18) is
also supported (626, 679) by increased functional connectivity of the
non-reward-related lateral orbitofrontal cortex (615,
626)
with the posterior
cingulate cortex (588)
which provides a dorsal route into the hippocampal memory system (584),
and decreased functional connectivity of the reward-related medial
orbitofrontal cortex with the parahippocampal gyrus (564)
which provides a ventral route into the hippocampal memory system, with
both effects enhancing sad and reducing happy memories in depression (615,
626, B16, B18).
A pregenual
/ subcallosal subdivision of the anterior cingulate cortex normally
with high connectivity with the medial orbitofrontal cortex reward system
has increased functional connectivity with the
lateral orbitofrontal cortex non-reward system in depression. This may provide a mechanism for more non-reward
information to be transmitted to the reward-related part of the
anterior
cingulate cortex, contributing to depression (596).
The amygdala has reduced functional
connectivity in depression (590).
The importance of the orbitofrontal
cortex, a key brain area for emotion, in depression (626)
is supported by an
activation study in the monetary incentive delay task (623).
This shows that the sensitivity of the lateral orbitofrontal cortex to
non-reward (not receiving an expected reward, a contingency that can
produce sadness) is higher in adolescents with a high severity of
depressive symptoms. Further, the medial orbitofrontal cortex is less
sensitive to reward in those with a high severity of depressive
symptoms (623).
This provides further key evidence relevant to the theory of
depression (559,
626,
B13, B14, B16, 679, B18).
An overview of the brain mechanisms of depression, and
how this fits in with understanding of the brain mechanisms of emotion (626, 674)
is provided in The Brain, Emotion,
and Depression (B13) and elsewhere (B18, 679, 631, 626). This approach
to depression has
implications for treating depression both psychologically and
medically (559, 626, 679,
B13, B14, B16, B18).
Depression, and
behavioural and depressive problems are associated in children with
sleep problems and with lower volumes of brain regions such
as the prefrontal cortex, orbitofrontal cortex, and anterior cingulate
cortex (616).
Lower volumes of these brain regions are also associated with
behavioural and depressive problems in children of mothers with
prolonged nausea and vomiting in pregnancy (622),
in children of young mothers (642),
and in children in families with family problems (636).
Childhood trauma is associated with mental health and cognitive
problems in adults, and the association is mediated by functional
connectivity of the orbitofrontal cortex, prefrontal cortex, and
temporal cortical areas (651, B18).
Schizophrenia
A theory of schizophrenia in which
reduced glutamate functionality in the prefrontal cortex destabilizes
attractor networks producing cognitive impairments in attention,
and exceutive function; and in which reduced glutamate function
in the orbitofrontal cortex leads to the negative symptoms. Increased
activity in medial temporal lobe networks overstabilizes attractor
networks there leading to the positive symptoms including
hallucinations and delusions (450,
490,
496,
503,
602,
B12, 631, B16, 681, B18).
The discovery in a sample of 2,567
patients with schizophrenia that the main variation between individuals
is in the negative symptoms, using the PANSS (580).
This has
implications for stratified treatment.
In first-episode
patients with schizophrenia the main changes in functional connectivity
involve the inferior frontal gyrus; and become established in thalamic
connectivity in the chronic state (563).
The temporal variability of functional connectivity is increased in
schizophrenia, is related to lower functional connectivity, and may
underlie the thought disorders (629).
Increased functional
connectivity of the precuneus and posterior cingulate cortex is related
to volition (thought control), and is not treated by neuroleptic drugs
(538).
In schizophrenia,
we provide evidence that goes beyond the disconnectivity hypothesis, by
showing in a large sample of people with schizophrenia that whereas the
effective connectivity in the strong or forward direction is reduced,
the effective connectivity in the weak or backward direction is not (602).
This may tend to result in over-emphasis on the internal world, with
relative disconnection from the reality of the external world (B16, B18).
Autism
A middle temporal gyrus / superior
temporal sulcus (STS) region involved in face expression processing and
theory of mind has reduced cortical functional connectivity with the
ventromedial prefrontal cortex which is implicated in emotion and
social communication. The precuneus, which is implicated in
spatial functions including of oneself, has reduced functional
connectivity. These two types of functionality, face
expression-related, and of one’s self and the environment, are
important components of the computations involved in theory of mind,
whether of oneself or of others, and the reduced connectivity within
and between these regions is proposed to make a key contribution to the symptoms of
autism (541,
570,
609, B18).
Obsessive-Compulsive Disorder
A theory
that hyperglutamergia in the prefrontal and premotor cortices in OCD
overstablizes attractor networks in these regions (449,
B14, B16, B18).
Effects of damage to the human
orbitofrontal cortex
Impairments
in the rapid reversal of associations between stimuli and reward value
in
patients with selective lesions of the orbitofrontal cortex and related
areas and
their relation to emotional changes (188, 203, 331, 354, B14, 641, B18).
Also, impairments in
impulsivity (353,
362,
394).
These discoveries were
inspired by the discoveries
on neuronal activity in the orbitofrontal cortex, and are relevant to
understanding
the changes in patients with frontal lobe damage and in patients with
borderline personality disorder (B16, B18).
A related discovery is of the effective connectivity
of the human orbitofrontal cortex, vmPFC and anterior cingulate
cortex, which shows how reward value and emotion can reach the
hippocampal memory system to become incorporated in episodic memory
(649, 657, B16, B18).
This also shows how these cortical regions have connectivity
with the septum and basal forebrain cholinergic systems, providing a
mechanism that may contribute to the memory impairments produced by
damage to the orbitofrontal cortex / vmPFC and/or anterior cingulate
cortex in humans (649, 657).
Addiction
The medial
orbitofrontal
cortex reward system has high functional connectivity in those who tend
to drink alcohol and who are sensation-seekers and impulsive; and
the lateral orbitofrontal cortex non-reward system has low functional
connectivity in those who tend to smoke, and are impulsive for a
different reason (599).
The medial orbitofrontal is also activated by amphetamine (367). These
discoveries underline the different neural bases for different types of
addiction (B14, B18).
Normal Aging
A theory
of how reduced stability of cortical attractor networks can
account
for some of the memory and cognitive symptoms of normal aging, with implications for treatment (540, 613, B16, B18).
Hypertension
and impaired memory
Even moderate hypertension is
associated with reduced hippocampal functional connectivity and
impaired memory (625, B18).
Brain, cognitive, and psychiatric differences associated with development
We have discovered a
constellation of somewhat similar functional and structural differences
of the brain (e.g. of the orbitofrontal cortex, anterior cingulate
cortex, and hippocampus) that are associated with lower cognitive
performance and with mental health symptoms including depression (B18). The
factors associated with these differences include childhood traumatic events ( 651), the family environment (636), low age of the mother (642), prolonged nausea and vomiting in pregnancy (622), and low sleep duration (616).
|